



by Yasser Omar Abdellatif and Ellie Graeden*
For most low and middle-income countries, global aid is a major source of funding for health security systems. Developing countries have been largely dependent on external support to sustain their vital functions. According to the UN, around 70 countries worldwide have been identified as aid-dependent. For example, in countries like South Sudan, Tuvalu, and Liberia, external financing accounts for more than 50% of GDP.
Such global aid helps improve education, bolsters social cohesion, and – pertinently –builds resilient health security systems to mitigate the impacts of infectious outbreaks such as Ebola, Zika, and cholera. With the proliferation of COVID-19 worldwide, fragile healthcare systems have become even more vulnerable, and therefore need immediate support to overcome the pandemic. We have learned from previous global pandemics that failing to respond effectively results in catastrophic economic and health consequences. So, have these countries gotten the support they need during this pandemic?
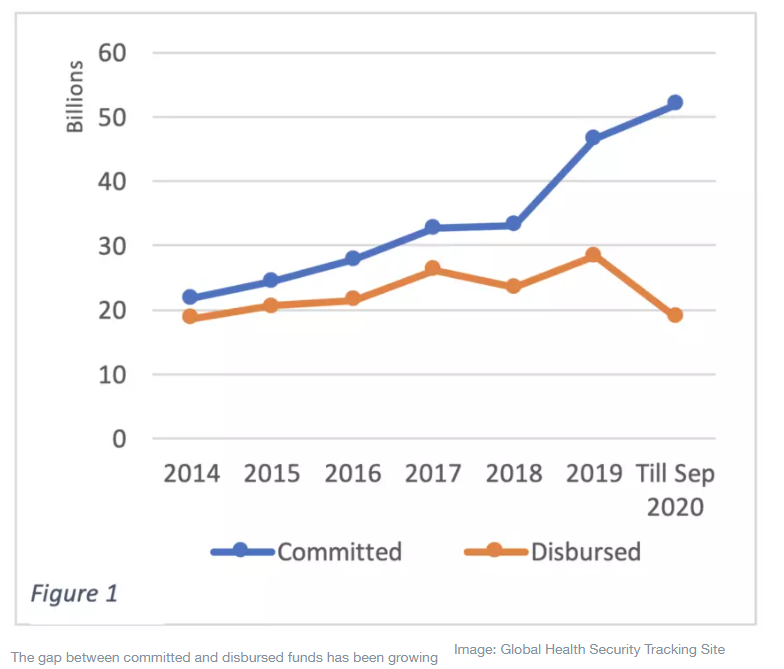
To answer this question, the Center for Global Health Science and Security at Georgetown University and Talus Analytics created the Global Health Security Tracking Site (GHSTS) to trace the flow of funding for health security around the world. According to GHSTS data, close to 80,000 projects have been funded since 2014 to support health security endeavours through global initiatives. As of September 2020, we recorded 456 projects engaged in efforts to counter COVID-19 globally. Total committed funds to support health security systems have increased (11%) this year compared to 2019. However, disbursed funds have declined significantly (34%), even after adjusting for projected disbursement for the rest of the year. In fact, the gap between committed funds and actual disbursed funds has been increasing over the last few years, as shown below in figure 1, indicating that there are barriers to committed funds being spent.
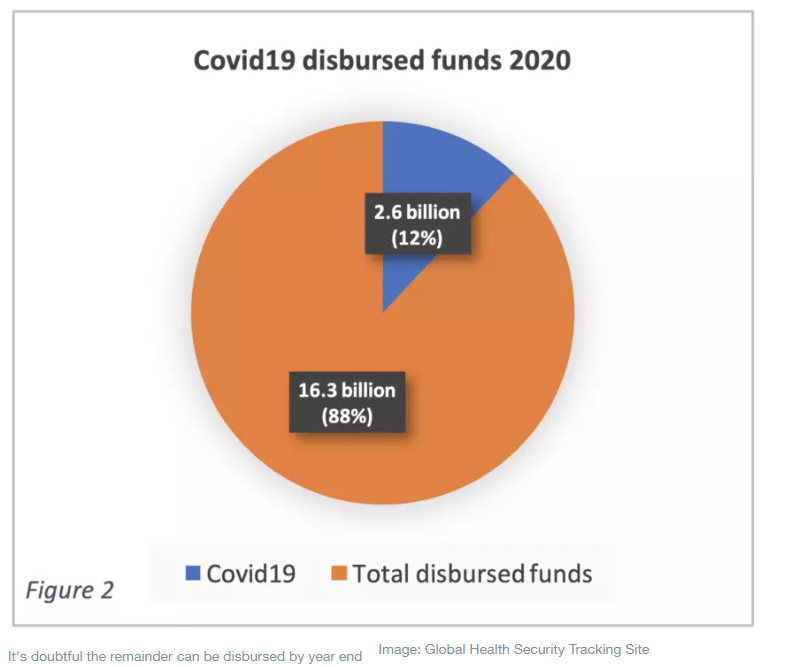
The amount of funds committed to COVID-19 related projects by donors in 2020 topped $22.5 billion, or about 30% of total committed funds earmarked for health security this year. However, only $2.57 billion were disbursed in the first eight months, or approximately 12% of total disbursed funds ($18.9 billion) - see figure 2 below. This gap raises doubts about the possibility of successfully disbursing the committed funds before the end of the year.
Decreasing global aid amid a global pandemic severely constrains efforts to control COVID-19 in countries with limited resources. For example, African countries have been struggling to provide enough testing due to limited lab capacity. This lack of testing, in addition to a lack of healthcare providers and lifesaving medical devices including ventilators, has likely cost the world hundreds of thousands of lives over the past few months. Additionally, as many economies have failed to mitigate the pandemic, 150 million people are expected to fall under the extreme poverty line by 2021, while the world income is expected to decline by 3% in 2020 – 6% below the initial expectations in January 2020.
Most of the funds for COVID-19 came from international organizations ($15.6 billion committed) and high-income countries ($5.1 billion committed). The World Bank Group is the largest donor of committed funds for COVID-19, announcing upwards of $12 billion in immediate support for country response. Japan is the second largest donor, committing the majority of their $1.6 billion in COVID-19 funding to the World Health Organization’s COVID-19 response. The European Union and International Bank for Reconstruction and Development (IRBD) came together in third place with $1.5 billion committed funds coming from each. Despite these commitments, we found that the International Bank for Reconstruction and Development disbursed more funds on COVID-19 related projects than any other funder at $523 million, followed by the UK, which disbursed around $400 million.
Tracking to whom and for what committed funds are designated, the data suggests that the majority of funding has been committed to response-specific activities, only some of which may contribute to building long-term health security and health capacity. Indeed, the data shows that the largest portion of funding ($12.3 billion) is allocated as ’general global benefit’, and is comprised primarily of the World Bank’s immediate response fund. The World Health Organization is the second highest recipient with $12.3 billion committed funds. Japan, Germany, Sweden, the EU and the UK are the main funders for the committed funds allocated to WHO to support their response plan for COVID-19. Coalition for Epidemic Preparedness Innovations (CEPI) is the third-top recipient for committed funds with $1.5 billion, and India ranked forth with $1.2 billion in committed funds. Of those receiving disbursed funds, the World Health Organization is on the top of list with $809 million; India has received $704 million and CEPI has received $192 million of estimated disbursed funds.
The lack of funds in support of global health security and preparedness systems amidst this global pandemic is substantially concerning. Donors have mobilized funds from other ongoing projects to create COVID-19 projects, suggesting these COVID-19-related efforts are drawing from funding efforts needed to support long-term capacity development and to address other critical health issues. In 2020, health security funds committed to Ebola have declined by 60% compared with 2019, while cholera funding was cut by 20%.
Defunding global health security efforts can cause long-lasting implications to global response towards any ongoing or potential future outbreaks that can cause similar severe global damage. Hence, the world must allocate adequate funds to countries in need to support their battle against COVID-19 without affecting their current health security projects. Additionally, more emergency funds are required now, more than ever, to make new COVID-19 vaccines available for people in low and middle-income countries. Otherwise, COVID-19 will remain a global threat and threaten our ability to prevent and respond to the next outbreak, causing loss of life as well as social and economic turmoil.
*Senior Research Associate, Center for Global Health Science and Security at Georgetown University and Associate Professor (Adjunct), Georgetown University
**first published in: www.weforum.org
 By: N. Peter Kramer
By: N. Peter Kramer

