


by Vasee Moorthy*
Most science fiction has tended to the dystopian view of the future. In these fictional dystopias the quality of life of the lower-income strata of society is often regressing, while the highest-income strata have access to technologies that render even ageing and death obsolete.
Back-casting is a method to work backwards from alternative future scenarios, and determine actions which can be taken now that influence which scenario comes to pass.
If we imagine a health dystopia in which the many promising health technologies are developed primarily for those with the highest incomes, while low-income settings lose out and potentially even regress, I here suggest three sets of actions that could shift society closer to a health utopia and away from a health dystopia.
1. Shift research to focus on the needs of the many
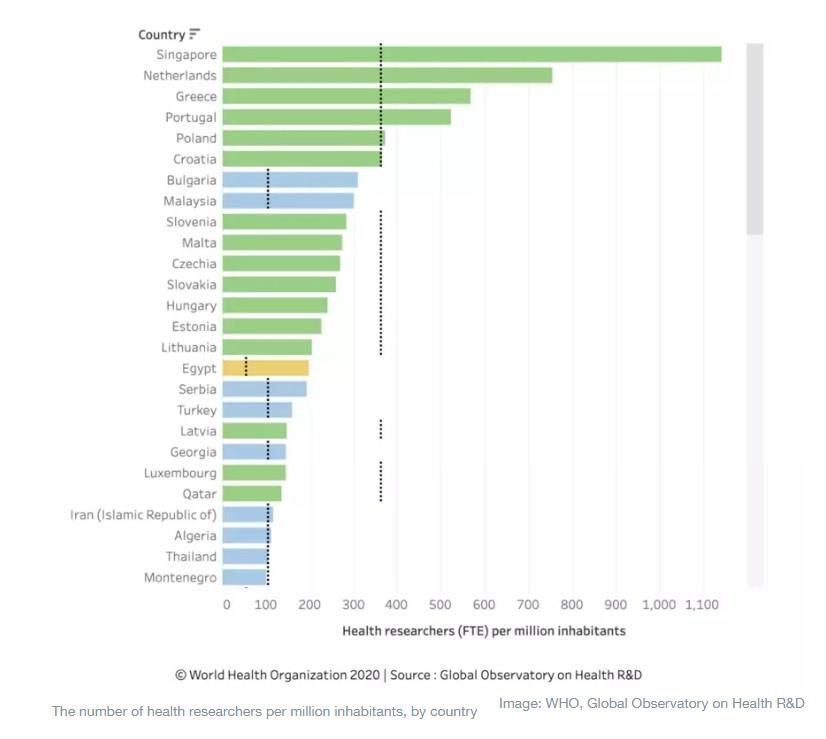
It has long been known that only a small percentage of worldwide research is devoted to the health problems of developing countries, where the great majority of the global disease burden is focused. There has been a movement in global health to try to reorient this imbalance. It has had partial success, including the establishment of major financing arms for the problems of the many such as GAVI and the Global Fund. The WHO’s Global Observatory on Health R&D highlights that less than 1% of grants from the leading health grant-making bodies globally are made to low-income countries, and even this tiny proportion of research grants focuses on areas that are not necessarily the priority concerns of those countries now. WHO’s R&D Observatory also highlights that high-income countries have an average of 73 times more health researchers per capita than low-income countries. While some countries have increased their funding on the health concerns of low and middle-income countries (LMIC), it is still the case that as little as 1% of all health R&D funding is spent on critical problems such as malaria and tuberculosis.
Precision or personalized medicine holds massive potential to shift focus from sick care to well care. Data on genetic predispositions, the biological basis of genetically determined conditions, lifestyle choices and exposures may in future be used to predict and intervene before disease occurs. But this depends on data being accessible for all types of ancestry and exposure. In practice the overwhelming majority of data is based on those of western European ancestry, and females are under-represented.
Machine learning algorithms will make predictions based on big datasets, but those predictions will be more often wrong if the underlying datasets are not representative. A concerted effort is needed to generate data in ethically appropriate ways so that the needs of underserved populations can be met.
An example of research that focused on the needs of the many would be significant investment in non-communicable disease (NCD) service delivery needs in low and low-middle income countries. There is an enormous and growing burden of years of healthy life lost to NCDs in lower-income settings. Affordable screening methods, tailored models for service delivery and access to diagnostics and medicines for diabetes, hypertension, common cancers, mental health and more effective surgical care are all badly needed in low-income settings. Implementing research into how best to deliver this care could be hugely valuable.
2. Incentivize product development for global medical needs
How do we define the need for health R&D? Simplistically we can make assessments of the health problems facing the world that require new medical advances. One can then review the pipelines or investment reports outlining health R&D activities. If we assess the difference between what is being developed and the needs, we see the gap, and in any analysis, huge gaps in R&D remain. Major gaps include R&D for diagnostics and therapeutics for the WHO list of neglected tropical diseases and for the WHO R&D blueprint priority list of epidemic diseases. Even bigger gaps are seen when assessing needs for products formulated to meet NCD screening and management needs in developing countries.
This is unsurprising when we review the drivers for health R&D. The market value of a medical product is based on the revenues and profits companies can expect to receive. This is directly related to the purchasing power of consumers and governments. There is no incentive to develop medical products for the poor outside the scope of the Global Fund and GAVI. An ecosystem of R&D funders disbursing public funds has emerged over the past 20 years to correct this gap on the push side; these are known as product development partnerships. These receive funds from donor countries and foundations and often base their funding on WHO’s assessments of unmet medical need. However, the size of investment is not close to the need. The total R&D funding for the year 2017 for all neglected infectious diseases was approximately $3.5 billion. In contrast, a single medical biotechnology product is thought to have generated about $20 billion in revenue in 2018 and the global alopecia market size for medical products is estimated to reach $4.8 billion annually by 2026, for an indication for cosmetic purposes. One estimate of the total health R&D spending by the private sector alone is $179 billion in 2018. This is not including government spending on health R&D, which is very large. The US National Institutes of Health alone spends over $30 billion of taxpayers money on health research. Total spending on the major needs for medical products (as defined by G-Finder) at the global level is less than 2% of overall spending.
An important related aspect is the great progress in the range of technologies that can be brought to bear for priority indications. For example, a recent clinical trial of ebola therapeutics indicated that two monoclonal antibody preparations were superior to the previous standard of care, and an ebola vaccine has been developed with >90% efficacy. While monoclonals, a form of biologically manufactured treatment or preventive option, are a big growth area for high-income country markets (the biggest selling drug in recent years is from this class), they have huge untapped potential for many diseases prevalent in LMICs. When we link the enormously promising pipeline of technologies to the medical need more systematically, we will be making progress.
Examples of success here would include greater focus on WHO’s priority R&D needs in neglected tropical diseases such as snakebite, schistosomiasis, human African trypanosomiasis, lymphatic filariasis and rabies. Snakebite is a good example of the poor priority setting that currently exists in global R&D. Hundreds of people die every day from snakebite envenoming. High quality, properly evaluated antivenoms are highly effective but are unavailable in many countries despite the fact that the technology to develop them has existed for decades. A needs-based R&D system would be working with great urgency to deliver affordable treatments for snakebite envenoming where needed around the world.
3. Don’t limit access due to affordability
Concerns about lack of reliable access to high quality, safe and effective products are so substantial that the World Health Assembly has called for a roadmap for Access to Medicines. Pricing of new medical products is on an inexorable rising trend which is rendering certain new drugs unaffordable even for some high-income countries. Our technologies have progressed to the point where we as a global community could decide to develop them for those most in need, or as is the current situation we can effectively restrict access to some high-income countries or individuals. If this trend continues we will have more and more treatments, but many of them will be unaffordable for those who need them most. A related ongoing trend will be financial hardships caused by becoming impoverished through paying for high cost treatments for family members.
There remains a fundamental disconnect between the very large amounts of investment that go into publicly funded R&D and the fact that many patients and countries cannot afford access to products developed as a result. A live example is now underway and we don’t yet know how it will end. COVID-19 R&D is receiving very substantial public and philanthropic funds. WHO and partners have initiated the Access to COVID-19 Tools accelerator as a global collaboration linking R&D with access. WHO is calling for collaborative approaches to science and global solidarity to facilitate equitable access.
Many problems, but many potential solutions if we recognize the risks and act
Any solutions must enable needs-based product development and new technology development to thrive in a sustainable manner. What is needed is a high-visibility initiative to look at where our current biotechnology development trends – if uncorrected – are taking us from a societal and equity perspective and then brainstorm openly on how we can course correct, including industry, academia, government and international agency voices. This discourse must occur with full participation of the private sector.
The past 20 years have seen huge progress in certain areas. GAVI and the Global Fund disburse billions of dollars per year of taxpayer and philanthropic funds. Twenty years ago, entities such as these may have seemed like an idealist’s dream. Is it beyond the capability of humanity to rise to equally huge gaps that the current system witnesses? What will be tomorrow’s GAVI, tomorrow’s Global Fund?
The two big ideas at the 2019 Global Futures Council on Biotechnology related to more effective models for therapeutics development and a new global initiative for advanced diagnostics, both areas with astonishing capabilities if technologies can be brought to bear on the world’s problems. My ask is that as we imagine these, we design systems based on global medical needs from the outset, placing equitable access to the products that arise right at the forefront. I am optimistic we can do it.
*Infectious diseases physician, immunologist, product developer, Science Division, World Health Organization
**first published in: www.weforum.org
 By: N. Peter Kramer
By: N. Peter Kramer
